
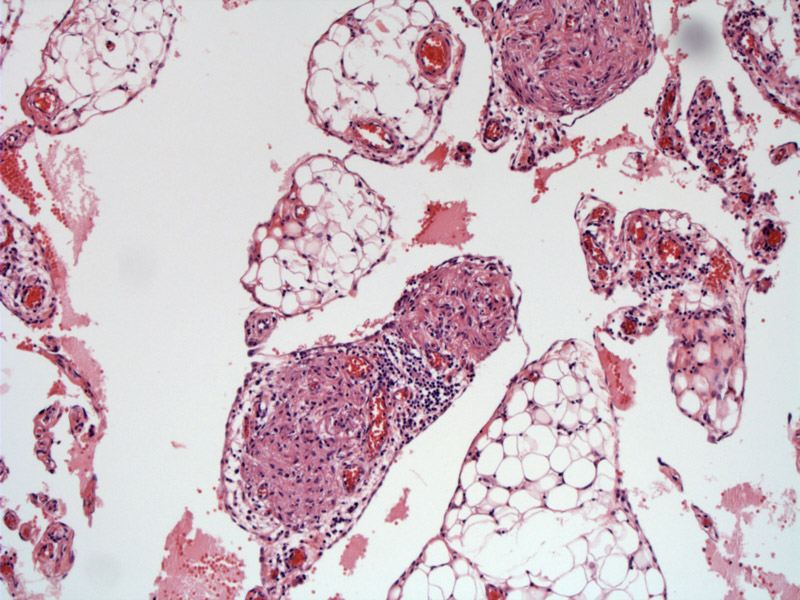
Normal lobules of omental fat are seen, and the architecture is not disturbed by the presence of scattered nodules of glial tissue.
The glial nodule is composed of orderly bundles of spindled cells.
A higher power view of mature-appearing glial tissue forming a fairly well-demarcated nodule in the omentum.
The glial nodule consists of cells with round to spindled nuclei set in a fibillary background. Scattered lymphocytes are also present.
Gliomatosis peritonei is characterized by implantation of nodules of glial tissue on the peritoneal surfaces of patients with mature or immature ovarian teratomas. It is important to recognize this entity as the greyish nodules can have a miliary pattern over the peritoneal surfaces because they may be mistaken for either peritoneal tuberculosis or peritoneal carcinomatosis (Muller).
DNA analysis demonstrates genetic differences (allelic variation) between the ovarian tumor and the glial implants, which suggests multiple independent tumors arising from submesothelial stem cells rather than true tumor recurrence/spread (Best, Ferguson).
Muller and colleagues (2002) conducted a review of all GP cases in the literature and found that 86 cases have been reported thus far. The glial nodules are usually composed of mature glial tissue 1-3 mm in diameter, but may be significantly larger (up to 3.5 cm). The average age at diagnosis is 15.4 years with a range 10 months to 46 years.
It appears the majority of gliomatosis peritonei remain asymptomatic and persist for many years without any changes. In some cases, they undergo fibroblastic transformation and disappear. In a subset of patients, they can transform into malignant glial or teratomatous tissue (e.g. glioblastoma multiforme) and lead to death (Muller).
Of the 86 cases reviewed by Muller and colleagues, 11 fatal cases were reported. The grade of the ovarian teratomas in these fatal cases were as follows: grade I (3), grade 2 (2), grade III (6). Thus, higher grade immature teratomas seem to predominate in situations where the glial implants become malignant.
Note that there are some differences between authors as how to grade immature ovarian teratomas, but mostly, higher mitotic activity and increased presence of immature elements (predominantly neuroepithelium) indicates a higher grade tumor (Muller).
Ferguson AW, Katabuchi H, Ronnett BM, Cho KR. Glial implants in gliomatosis peritonei arise from normal tissue, not from the associated teratoma. Am J Pathol. 2001 Jul;159(1):51-5.
Kwan MY, Kalle W, Lau GT, Chan JK. Is gliomatosis peritonei derived from the associated ovarian teratoma? Hum Pathol. 2004 Jun;35(6):685-8.
Müller AM, Söndgen D, Strunz R, Müller KM. Gliomatosis peritonei: a report of two cases and review of the literature. Eur J Obstet Gynecol Reprod Biol. 2002 Jan 10;100(2):213-22.

){kind=link}
){kind=link}
){kind=link}
){kind=link}