
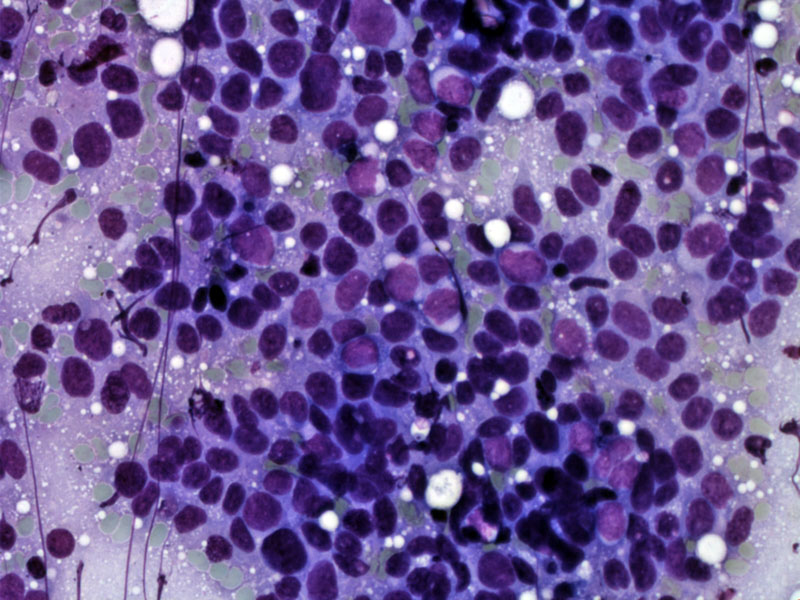
Smears from an FNA show a cellular neoplasm with many single cells without distinct nucleoli.
){kind=link}
This smear shows the delicate uniform chromatin which defines this entity.
){kind=link}
Areas of nuclear molding can be appreciated.
){kind=link}
Irregular large nests of tumor cells with scant cytoplasm are seen. There is prominent central comedonecrosis.
){kind=link}
Around a vessel are relatively uniform cells with scant cytoplasm and finely stippled salt and pepper chromatin. Nuclear molding is appreciated. The neoplastic cells are approximately three times the size of lymphocytes.
){kind=link}
Another tumor shows anastomosing ribbons of cells with scant cytoplasm.
){kind=link}
Cells show salt and pepper chromatin and focal nuclear molding.
){kind=link}
Extensive lymphovascular invasion is not an uncommon feature of this tumor.
){kind=link}
Strong diffuse staining for keratin AE1/3 is present.
){kind=link}
Synaptophysin, shown here, or chromogranin, or both are frequently present.
){kind=link}
Staining for CD56 is less intense but not infrequently involves the majority of cells.
){kind=link}
Nuclear TTF-1 staining is seen here throughout the tumor.
){kind=link}
CT scan shows a distinct lung mass with spiculation.
){kind=link}
Imaging of the brain small cell carcinoma which has a tendency to metastasize to the brain as seen here.
){kind=link}
The brain biopsy shows small cell carcinoma infiltrating the normal brain parenchyma.
){kind=link}
Small cell carcinoma, also known by the older term oat cell carcinoma or the newer term poorly differentiated neuroendocrine carcinoma, comprises about 12-25% of all lung cancers and is strongly associated with smoking (Cheng). Microscopically, the small round blue cells usually grow in diffuse sheets with nuclear molding and indistinct cell borders. The common neuroendocrine formations (trabeculae, periphery pallisading, rosettes) may occasionally be seen, especially if a moderately differentiated neuroendocrine tumor (atypical carcinoid) has transitioned into poorly differentiated small cell carcinoma. The nuclei exhibit "salt and pepper" chromatin with indiscernible nucleoli. There may be crush artifact leading to basophilic stippling staining of vessel walls called "Azzopardi effect". Mitotic activity is brisk and necrosis can be extensive.
IHC studies reveal positivity for chromogranin, synaptophysin, CD56/NCAM and low molecular weight keratins. 85% express positive nuclear TTF-1 staining (Zander), and this along with p63 negativity in SCC may be helpful in differentiating small cell carcinoma from poorly differentiated squamous cell carcinoma (Fletcher).
Occurs in adults between ages 40-70, and usually arises in a central location (70% present as a perihilar mass). There is usually spread to regional lymph nodes and the mediastinum by the time of diagnosis. Hemoptysis, hoarseness, paralysis of the vocal cords and superior vena cava syndrome may be presenting symptoms, as well as paraneoplastic syndrome such as SIADH, Cushing syndrome and Eaton-Lambert syndrome.
Patients with limited-disease represent approximately 30% of all patients with SCLC, and are potentially curable. Combination chemotherapy is the cornerstone of treatment for both limited and extensive disease. Surgery can be considered but is reserved for those with a solitary pulmonary nodule.
Highly aggressive tumor that metastasizes early. The usually TNM stage is less useful due to the rapid growth of this tumor, thus, small cell carcinoma is broadly divided into "limited" or confined to one hemithorax, or "extensive" stage disease, where metastases to bones, liver and brain have occurred.
• Salivary Gland : Small Cell Carcinoma (of parotid)
• Endometrium : Small Cell Carcinoma
• Lung : Large Cell Neuroendocrine Carcinoma
• Bladder : Small Cell Carcinoma
• Neuroendocrine : Merkel Cell Carcinoma
Cheng L, Bostwick DG, eds. Essentials of Anatomic Pathology. 2nd Ed. Totowa, NJ: Humana Press; 2006: 948.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 189.
Zander DS, Farver CF. Pulmonary Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2008: 563-6.