
The epidermis shows irregular acanthosis with parakeratosis, while the superficial dermis has a smattering of lymphocytes and vertically oriented collagen fibers.
){kind=link}
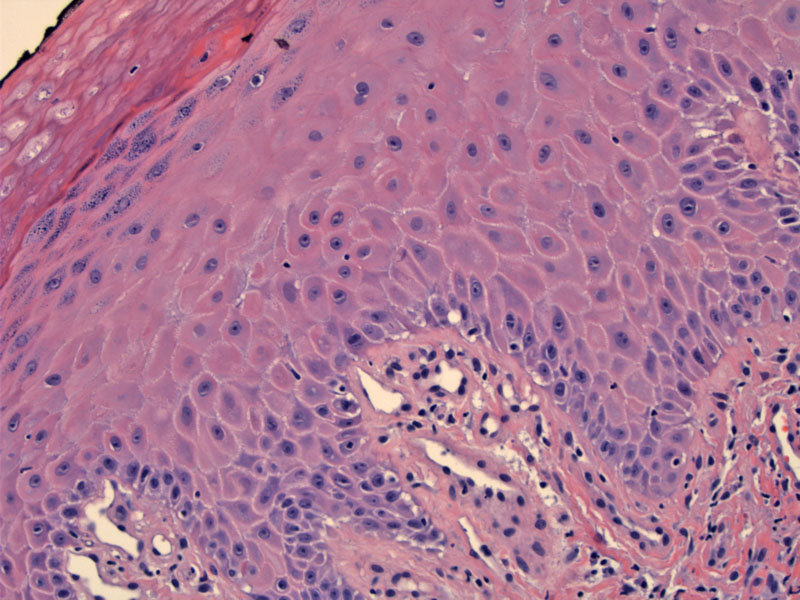
This is another case of LSC, which demonstrates focal parakeratosis, irregular acanthosis (note the jagged rete ridges) vertically oriented collagen in the papillary dermis. Note also the presence of pigment incontinence, intraepidermal spongiosis (as demonstrated by visible intercellular bridges between keratinocytes) and hypergranulosis (most prominent in the superficial layers of the epidermis in the upper right).
){kind=link}
Clinically, LSC is a scaly erythematous plaque. In this case where the intertriginous zones were affected, there is superimposed ulceration.
){kind=link}
Lichen simplex chronicus (LSC) is a scaly erythematous plaque that develops in response to constant rubbing. Most commonly affected sites include the perianal and genital regions, as well as the posterior neck, forearms and pretibial areas. The underlying cause of pruritis is unknown, although patients with a history of atopy are more prone to developing LSC.1
Note the LSC is lichenoid clinically, but does not exhibit a lichenoid pattern of inflammation histologically. Microscopically, there is hyperkeratosis, focal areas of parakeratosis and hypergranulosis. The rete ridges display irregular jagged acanthosis (versus regular acanthosis with broad rete ridges seen in psoriasis). The papillary dermis demonstrates "vertical streaks" of eosinophilic collagen bundles. Perivascular infiltrate is common. Lymphocytes and spongiosis may be seen in the epidermis.
Pruritic scaly thickened plaques develop at affected sites as a result of chronic rubbing. Superinfection may occur if the scratching leads to ulceration and abrasion.
Treatment is targeted toward cessation of scratching. Topical emollients and steroids may be used.
→LSC is lichenoid (scaly plaque) clinically, but NOT histologically i.e. there is no lichenoid infiltrate.
→Vertical orientation of collagen in dermal papillae is a key histologic feature.
→LSC is usually due to chronic rubbing or scratching; the initial stimulus may be an insect bite, nervous habit/stress, eczema or some sort of irritation.
1 Nucci MR, Oliva Esther. Gynecologic Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier: 2009: 23-4.
2 Rapini RP.Practical Dermatopathology. Philadelphia, PA: Elsevier; 2005: 48-9
Clinical photo courtesy of Dr. Alan Waxman, Dept of Obstetrics and Gynecology, University of New Mexico.