System: Breast: Ductal: Indeterminant: Flat Epithelial Atypia

System: Breast: Ductal: Indeterminant: Flat Epithelial Atypia

1 Image
2 Image
3 Image
4 Image
5 Image
6 Image
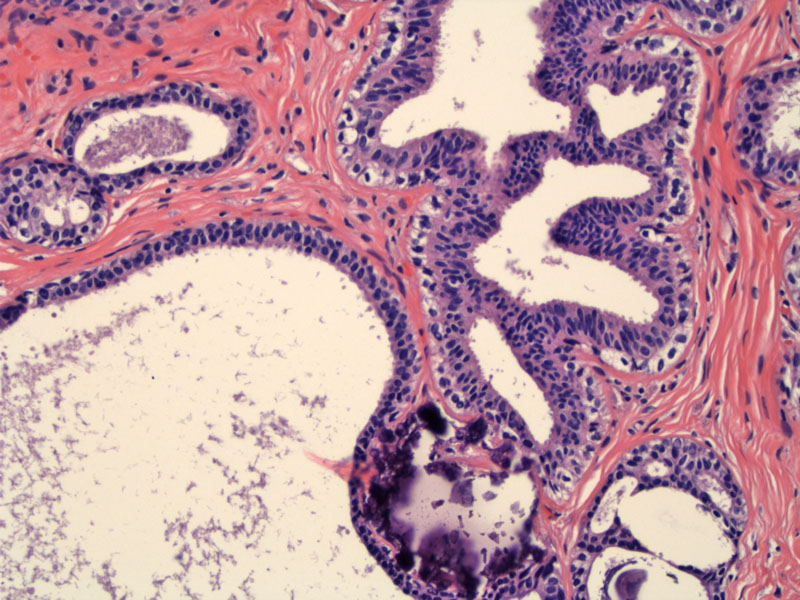
Columnar cell lesions encompasses a spectrum of changes including columnar cell change (CCC), columnar cell hyperplasia (CCH) and flat epithelial atypia (FEA). To simply matters, one might divided columnar cell lesions into two main categories: non-atypical/uncomplicated and atypical. Non-atypical columnar cell lesions include CCC and CCH. Please refer to our other case for columnar cell lesions for more details on these entities.
Atypical columnar cell lesions (aka CCC or CCH with atypia) have been coined a new name 'flat epithelial atypia' by the WHO Working Group on Pathology and Genetics of Tumors of the Breast in 2003. FEA demonstrates features CCC or CCH, but with cytological atypia defined as the following: a change in nuclear shape from elongated (found in CCC or CCH) to round and ovoid, mildly increased N:C ratio, variably prominent nucleoli, slight margination of chromatin and loss of polarity.1,2
In comparison, CCC and CCH should consist of nuclei that are elongated and oval with even chromatin and inconspicuous nucleoli. Furthermore, these epithelial columnar cells are well-oriented (perpendicular to the basement membrane).
Note also, that FEA lacks the architectural constructs (cellular bridges, arcades and fenestrations) typically found in atypical ductal hyperplasia or DCIS; hence the term flat epithelial hyperplasia. The degree of cytological atypia in FEA is mild to moderate. If there is high-grade atypia, the diagnosis is DCIS even if there is only a single cell layer.
FEA cannot be detected grossly, but are increasingly encountered in biopsies performed for mammographically detected calcifications.
If FEA is identified on core-needle biopsy specimens then excisional biopsy is required. When FEA is identified in an excisional biopsy specimen, then multiple levels are required to look for features diagnostic of ADH or DCIS; one may also submit the remainder of tissue.
FEA is an area of active investigation, but it appears that these are pre-neoplastic lesions that may represent early forms of DCIS or invasive carcinoma. Studies have shown an association of FEA with ADH, low-grade DCIS, tubular carcinoma and lobular neoplasia (ALH or LCIS). Therefore, if a pathologist identifies FEA in a specimen, he or she should perform a diligent search for these other aforementioned lesions by obtaining additional levels or blocks containing the lesion and by the submission of the remainder fo the breast tissue for histologic examination.
Despite a close relationship with neoplastic lesions, the few follow-up studies conducted thus far have shown that FEA (as an isolated lesion) has a very low likelihood of progression into invasive breast cancer.2 However, further research is required to better defined these lesions and categorize their risk.
1 O'Mallye FP, Pinder SE. Breast Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2006:151-7.
2 Collins LC, Goldblum JR eds. Current Concepts in Breast Pathology: Surgical Pathology Clinics. June 2009(2) No 2:263-272.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}