
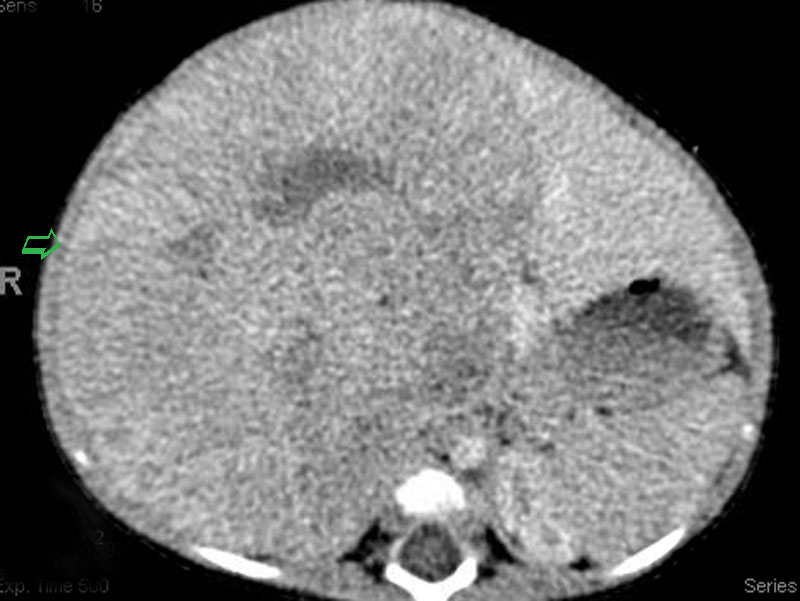
CT scan shows a massive liver based heterogenous rounded lesion containing several internal calcifications.
){kind=link}
The fetal pattern displays alternating areas of light and dark staining cells showing hepatoid differentiation. Normal portal triads are absent.
){kind=link}
The tumor cells form cords which may be up to 3 cells thick, recapitulating normal liver.
){kind=link}
Hepatoblastoma (HB) is the most common malignant liver tumor in the pediatric population. The vast majority of cases occur in children below age 5, with 68% of cases occuring before age 2 (Correa).
Grossly, HB presents as a large, single, well-circumscribed and multilobulated mass. Most masses are in the right lobe. Histologically, HB exhibits a myriad of patterns since the tumor recapitulates liver development through the various stage of development.
HB can be divided into two main subtypes: epithelial and epithelial-mesenchymal. The epithelial category is further subdivided into pure fetal histology (sheets or cords of fetal hepatocytes in an alternating light and dark pattern, which is caused by the amount of glycogen and lipid in the cytoplasm), embryonal histology (immature cells with basophilic cytoplasm arranged in cords, ribbons, rosettes, tubules) and less commonly, a macrotrabecular and undifferentiated small cell pattern (Fletcher, Correa).
The epithelial-mesenchymal pattern is composed of epithelial patterns in conjunction of msechemyal elements (e.g. immature fibrous tissue, osteoid, cartilege). In some of the cases, there may be teratoid elements (e.g. intestinal-type epithelium, squamous epithelium, skeletal and/or neural tissue).
Presents as an abdominal mass, weight loss and jaundice. In rarer cases, can present as precocious puberty since the tumor can elaborate hCG hormone. Serum AFP is elevated and can be a useful marker for recurrence after resection (Fletcher).
The incidence of HB appears to be rising, attributed to the increased survival of premature infants. There is an association with congenital syndromes such as Beckwith-Wiedemann syndrome and FAP (familial adenomatous polyposis). In fact, FAP (APC gene mutations) carries a 847x risk of developing hepatoblastoma.
Excision, with preoperative chemotherapy to shrink tumor in some cases.
The histologic types are subdivided into favorable (pure fetal histology with less than 2 MF per 10 HPF), less favorable (pure fetal histology with more than 2 MF per 10 HPF, combined fetal and embryonal, macrotrabecular, epithelial-mesenchymal) and unfavorable (small cell undifferentiated).
Staging is also very important and is based on the extent of residual tumor after surgery.
→Most common malignant liver tumor in children.
→Association with Beckwith-Wiedemann syndrome and familial polyposis coli (FAP). FAP carries an over 800-fold risk of developing hepatoblastoma.
→Many histologic patterns, broadly grouped into epithelial (fetal, embryonal, macrotrabecular, small cell undifferentiated) and epithelial-mesenchymal patterns.
→Small cell undifferentiated is the only pattern that is designated as unfavorable histology, the remainder are either favorable or less favorable.
Correa H. Hepatoblastoma. Pathology Case Reviews 2009;14:21-7.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 433-5.