System: Breast: Biphasic: Benign: Fibroadenoma


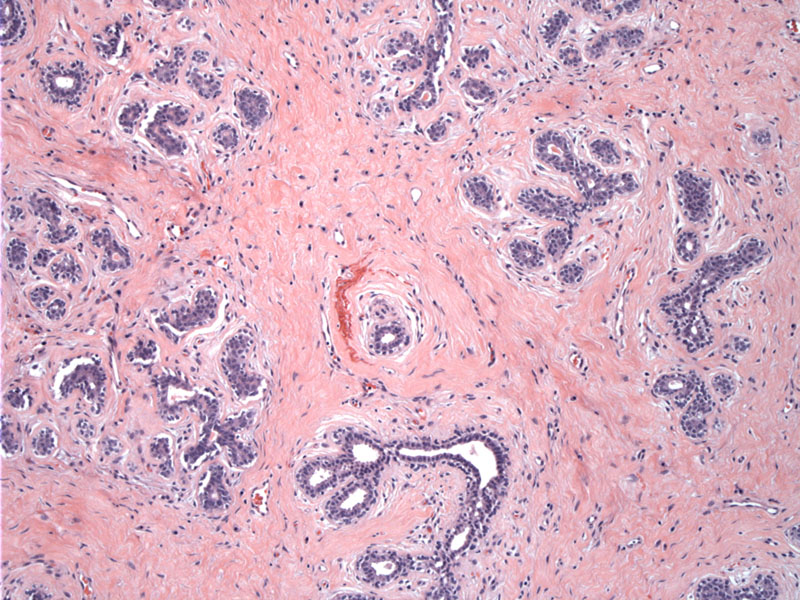
Case 1: The stroma is more hyalinized in this case, surrounding ducts in a pericanalicular pattern.
Case 2: This case demonstrates a myxoid stroma.
The ducts have the usual bilayer consisting of epithelial and myoepithelial layer. Proliferation of bland stromal cells surround ductular structures.
Case 3: The ducts in this case are ectatic with mild hyperplasia.
The epithelial hyperplasia is mild and without atypia. The stroma is also bland, without increased cellularity.
Fibroadenomas of the breast are benign fibroepithelial lesions composed of hyperplastic stromal and hyperplastic epithelial elements. Though often categorized as a neoplasm, it is now believed that fibroadenomas are polygonal hyperplastic overgrowths of hormonally-responsive stromal and epithelial elements (Fletcher).
Grossly, fibroadenomas are round or ovoid gray-white firm, well-circumscribed masses. The cut surface is rubbery, lobulated and sometimes myxoid. In older women, the mass may be hard, sclerotic and calcified (Fletcher). Similar to fibroids of the uterus, they can be "shelled out" from the surrounding breast tissue. Typically, they are 1-3 cm in size, but in some instances (especially in younger women), they may grow rapidly and exceed 20 cm in size and thus are termed "juvenile" or "giant" fibroadenomas (O'Malley).
Microscopically, loose cellular stroma surrounds ductular structures. The stromal cells are spindled and uniform. The stroma can be myxoid, or hyalinzed and calcified (especially in older women). The ductules have two distinct patterns, intracanalicular (cleft-like) and pericanalicular (ductules are rounded and tubular). Both the intracanalicular and pericanalicular may be seen in together, and there is no prognostic significance to these patterns (Fletcher).
Epithelial hyperplasia may be seen in the epithelial component, especially in juvenile fibroadenoma and should not be overcalled as atypical ductal hyperplasia. In very rare instances, the epithelial may exhibit changes consistent with atypical ductal hyperplasia, LCIS or DCIS, but one must be very very careful in making this diagnosis (Fletcher, O'Malley).
These are common tumors that present as mobile, painless and well-defined lumps, especially in younger women (20s and 30s). In older patients, the lesion can be fibrous and sclerotic. Since fibroadenomas are hormonally responsive, some enlarge during pregnancy and regress afterwards. Occasionally, the fibroadenoma infarcts and is worrisome for malignancy. Many lesions become atrophic after menopause (O'Malley).
The main differential diagnosis is phyllodes tumor. The stroma of fibroadenoma is uniform and lack pleomorphic features and mitoses, but in some cases, it may be very difficult to distinguish between the two.
• Biphasic : Juvenile Fibroadenoma
• Biphasic : Malignant Phyllodes
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 906-7.
O'Malley FP, Pinder SE. Breast Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elvesier; 2006: 109-116.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}