
This portion of pelvic bone contains a 15 cm tumor involving the medial musculature and acetabulum. The tumor is tan, whorled, and has bluish-white areas compatible with cartilagenous growth while other areas are more tan and fleshy -- a bimorphic appearance suggests the diagnosis.
){kind=link}
A lobulated well-differentiated proliferation of neoplastic chondrocytes exhibits features of a grade I or grade II chondrosarcoma.
){kind=link}
Juxtaposed to the areas of low-grade chondrosarcoma is an undifferentiated high grade sarcoma. This high grade sarcoma area can be spindle cell sarcoma, osteosarcoma, or even rhabdomyosarcoma.
){kind=link}
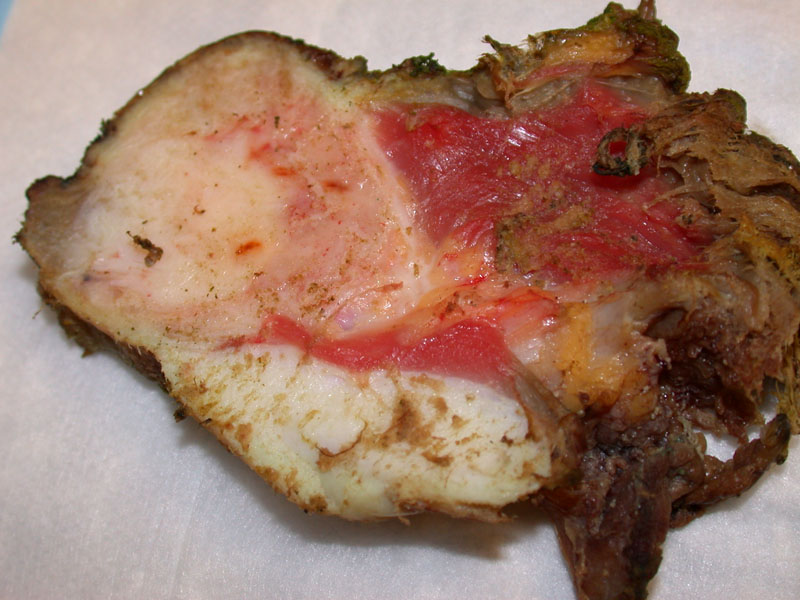
This nice series of gross photos of dedifferentiated chondrosarcoma are courtesy of Dr. David Hicks at University of Rochester. A glistening cartilagenous tumor has areas which invade into the surrounding soft tissue.
){kind=link}
A closer look at the biphasic appearing tumor with a soft tissue component.
){kind=link}
Features characteristic of classic chondrosarcoma are juxtaposed to a destructive component. Both cartilaginous (white, glistening) and sarcoma (fleshy and tan) components can be seen.
){kind=link}
In the calcaneus, there is an chondrosarcoma with underlying bone invasion arising the superior portion of the cortex.
){kind=link}
Another closer look of the prior image. The more chondroid appearance of the surface tumor contrasts wthe variegated fleshy nature of the high grade component.
){kind=link}
In terms of location, dedifferentiated chondrosarcoma occurs in the same places as conventional chondrosarcoma (e.g. shoulder, pelvic girdle). Radiologically, the classic features of chondrosarcoma (e.g. thickened cortex, expansion of bone, lucent areas admixed with irregular calcifications) are seen, however, there will be an abrupt transition to a more destructive area. This is reflected histologically where there will be an area of typical low-grade chondrosarcoma juxtaposed to a high grade sarcomatous lesion.
The low-grade chondrosarcoma component is typically grade I or grade II. The sarcomatous component is high-grade and may exhibit features of a leiomyosarcoma, fibrosarcoma, rhabdomyosarcoma or simply a pleomorphic sarcoma.
The key differential diagnostic consideration is a chondroblastic osteosarcoma. The latter occurs in young adults whereas chondroblastic osteosarcoma arises in older adults. Furthermore, the spindled component merges with the chondroid component whereas in dedifferentiated chondrosarcoma, the two components are sharply demarcated. The chondroid component is much more malignant-appearing in chondroblastic osteosarcoma compared to dedifferentiated chondrosarcoma. Of note, dedifferentiated chondrosarcoma has a much worse prognosis than chondroblastic osteosarcoma, so it is important to make this distinction (Fletcher).
Compared to conventional chondrosarcoma, dedifferentiated chondrosarcoma arises in patients who are 10 years older. The pelvis and femur are the most common sites of involvement.
Surgical excision with clear margins. These tumors are rather chemo-resistent.
Recurrence is frequent. Overall prognosis is poor, with a five year survival of only 13% (Mercuri). Correct diagnosis is more important than classification of the dedifferentiated
component, since this may behave very differently from the primary sarcoma which it resembles.
→Dedifferentiated chondrosarcoma is composed of a low-grade chondrosarcoma juxtaposed to a high grade sarcoma.
→The key differential diagnostic consideration is chondroblastic osteosarcoma.
• Chondroid : Chondrosarcoma, Myxoid Type
• Osseous : Chondroblastic Osteosarcoma
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 1611-2.
Mercuri M, Picci P, Campanacci L, Rulli E. Dedifferentiated chondrosarcoma. Skeletal Radiol 1995;24:409-16.
We thank Dr. David Hicks of University of Rochester for his contribution of gross photos to this case.