System: Skin: Vascular: Vascular: Superficial lymphatic malformation


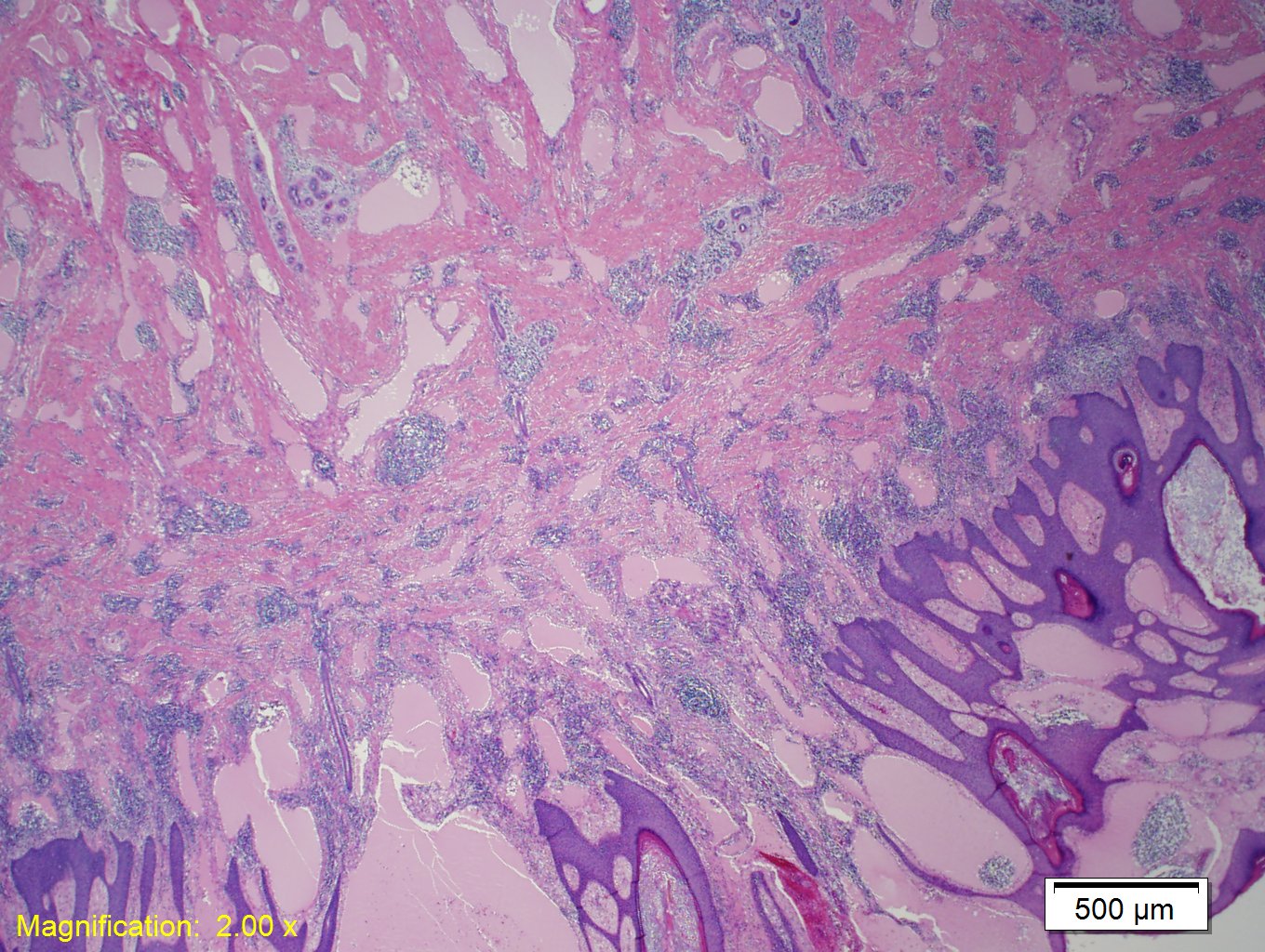
Case 1: A collection of dilated lymphatic vessels, filled by eosinophilic proteinaceious lymph, is located in the papillary dermis and extends into the dermis and subcutaneous tissue.
Slightly higher power view showing lyphatic vessels extending into the papillary dermis with overlying hyperkeratosis, often causing a verrucous appearance of the skin clinically.
Clusters of the lymphatic vessels in the papillary dermis are responsible for the
High power view showing the lymphatic vessels lined by a single layer of flat endothelial cells. There is atrophy of the epidermis directly over the lymphatic vessels.
Superficial lymphatic malformation (lymphangioma circumscriptum , superficial lymphangioma, superficial microcystic lymphatic malformation) is in the family of lymphatic malformations that includes superficial lymphatic malformations, deep lymphatic malformation (cystic hygroma), and lymphangiomatosis. There terms lymphagioma and lymphangioma circumscriptum are often used to describe this lesion, however there are inaccurate terms according to Sangueza.
These lesions are fairly rare, making up 4% of all vascular tumors and 25% of all benign vascular tumors in children. In the United States, it is estimated that the incidence rate is 1.2-2.8 per 1000 live births with about 50% being present at birth and 90% appearing by age 2 (Patel).
The pathogenesis has been well described by Whimster et al., but entails abnormal lymphatic cisterns that grow independently from the normal lymphatic vessels deep in the subcutaneous tissue during development. These cisterns connect with the ectopic lymph vessels of the skin and result in the superficial appearance of vesicles.
These lesions generally present at birth or early childhood. The axilla, shoulders, neck, proximal extremities, and tongue are the most common site involved. These lesions have been referred to as “frog spawn” or “frog egg” of the skin for their clinical appearance consisting of clusters of numerous small vesicular like lesions that range in color from pink to red to black (presence of blood vessels or hemorrhage). Often there is hyperkeratosis or verrucous changes giving the lesion a thickened or plaque like appearance.
These lesions usually do not require treatment unless the patient requests it for a cosmetic reason, or if there is pain and discomfort associated with the lesion. Surgical resection is an option, but the lesions often recur given they frequently have a deep seated cistern supplying the superficial lesions. Argon and carbon dioxide lasers have been used to improve the cosmetic appearance of lesions successfully.
Patel GA, Schwartz RA. Cutaneous lymphangioma circumscriptum: frog spawn on the skin. Int J Dermatol. 2009;48:1290-5.
Requena L, Sangueza OP. Cutaneous vascular anomalies. Part I. Hamartomas, malformations, and dilation of preexisting vessels. J Am Acad Dermatol. 1997;37:523-49.
Whimster IW. The pathology of lymphangioma circumscriptum. Br J Dermatol. 1976;94:473-86.
){kind=link}
){kind=link}
){kind=link}
){kind=link}