System: Skin: : Indeterminant: Cutaneous Sarcoidosis

System: Skin: : Indeterminant: Cutaneous Sarcoidosis

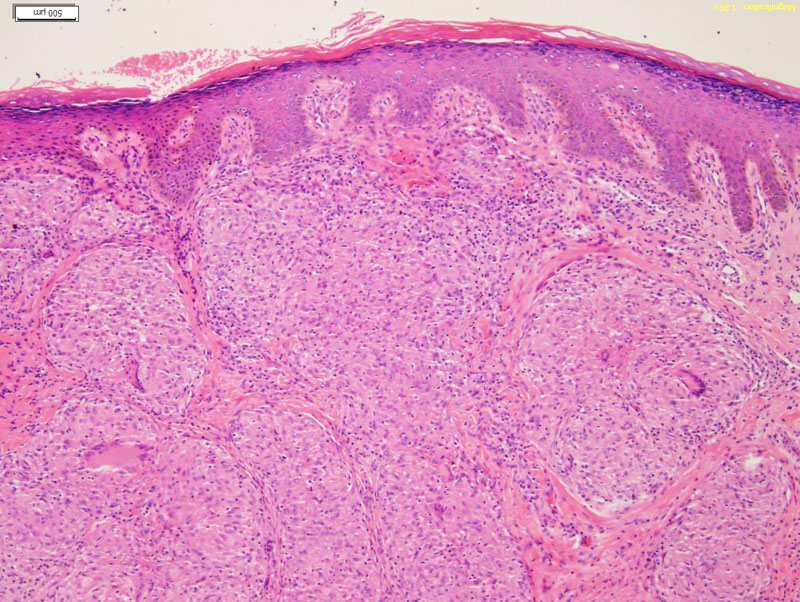
some keratosis and irregularity to the epidermis, underneath is the lesion Image
large back to back epithelioid granulomas, some multinucleated cells, invested in collagen Image
Sarcoid can affect any organ, with a preference for the lungs, eyes, lymph nodes and skin. Skin involvement occurs in between 20% to 35% of patients with systemic disease but may also occur by itself.
I copied this so it needs to be modified: ERYTHEMA NODOSUM
Sarcoidosis is only one of many causes of erythema nodosum, which is thought
to be a reactive phenomenon. Typically ill-defined tender, red nodules arise on
the limbs and resolve over 2 to 3 weeks with characteristic bruising (figure 1).
Erythema nodosum is classically seen in young women as a marker of acute
sarcoidosis.6 It is often seen in association with arthralgia, general malaise and
bilateral hilar lymphadenopathy on chest X-ray.
MACULOPAPULAR SARCOIDOSIS
Lesions arise as asymptomatic macules and papules ranging in colour from redbrown
to purple and in size up to 5 mm (figure 2). The commonest areas of
involvement are the face and extensor aspects of the limbs. Spontaneous resolution
may occur with or without atrophic scarring.
NODULAR SARCOIDOSIS
This form predominantly affects the proximal limbs and face. It is characterised
by the development of well-circumscribed nodules measuring more than 5 mm
across (figure 3). Again, the colour may vary from red-brown to violaceous and
there may be surface telangiectasia. Lesions tend to be indolent.
ANNULAR SARCOIDOSIS
Annular forms of cutaneous sarcoidosis are well recognised.7 Lesions of maculopapular
sarcoidosis often show annular formations. A more severe variant,
often occurring on the face and resembling necrobiosis lipoidica, is also seen.
Disfiguring circinate lesions arise with a leading granulomatous edge and a central
atrophic area with telangiectasia (figure 4). This form tends to be persistent.
SCAR SARCOIDOSIS
Granulomatous infiltration of scars by sarcoidal tissue may occur in a number of
situations, eg, surgical scars, at vaccination sites, and in tattoos.8 Scars become
infiltrated and inflamed with a violaceous colouration (figure 5). Scar sarcoidosis
activity may parallel systemic disease behaviour,5 but may also occur in isolation.
LUPUS PERNIO
This is more common in older patients and women.9 The face and nose are usually
involved with the development of infiltrated blue-red plaques and nodules
(figure 6). Lupus pernio is usually associated with chronic sarcoidosis, especially
involvement of the upper respiratory tract, lacrimal glands and bone. The
cosmetic effects of lupus pernio may be severe and lead to considerable psychological
distress.
PLAQUE SARCOIDOSIS
This indolent form of the disease usually involves the limbs with diffuse plaques. Again, these lesions may show similar features to the atrophic plaques
of necrobiosis lipoidica.
RARE FORMS
Other manifestations of cutaneous sarcoidosis which have been described
include nail involvement (figure 8) and angiolupoid, ulcerative, subcutaneous,
icthyosiform, psoriasiform, and lichenoid forms.
With the exception of erythema nodosum and maculopapular sarcoidosis, most
of the types of cutaneous sarcoidosis are chronic.
){kind=link}
){kind=link}