System: Endocrine: Thyroid: Metabolic: Amyoid Goiter


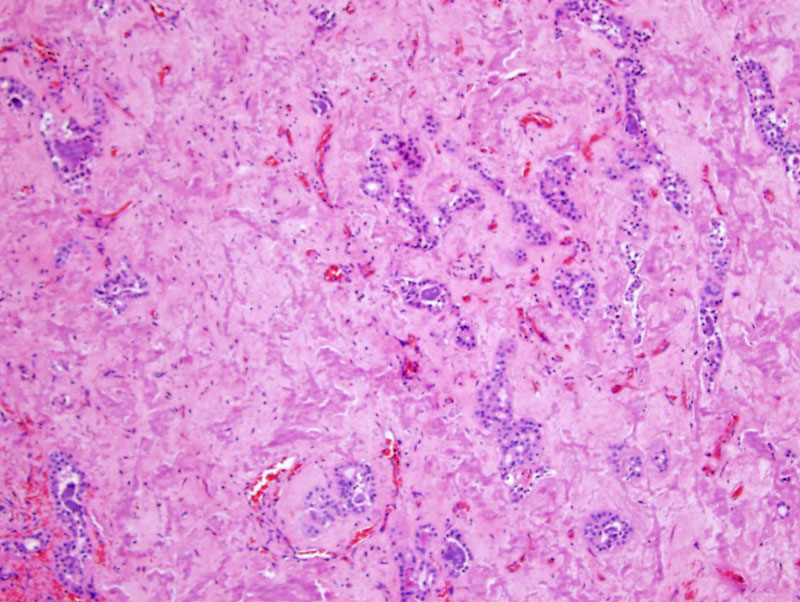
Case 1: Amorphous deposits of amyloid infiltrate after the remnants of thyroid parenchyma.
The normal follicular epithelium is disrupted and surrounded by amyloid.
Congo red staining highlights the amyloid. Apple-green birefringence (not shown here) would support the diagnosis.
Case 2: Again, note the amyloid deposits around the follicles.
Waxy eosinophilic material encasing the acini can be appreciated.
Amyloid goiter is a very rare occurence, but can be seen in in long-standing inflammatory diseases (chronic infection or inflammation); in this instance, the amyloid is usually of the AA type. Amyloid goiter due to plasma cell abnormalities would have AL type amyloid.
Grossly, the thyroid is enlarged with a white-tan to salmon-colored appearance on the cut surface. Microscopically, deposits of amyloid are seen surrounding follicles. Congo red staining with pple-green birefringence (upon polarization) would confirm the diagnosis.
Presents with bilateral thyroid enlargement; patients may have amyloidosis of other organs.
Lloyd RV, Douglas BR, Young WF Jr. Endocrine Diseases: Atlas of Nontumor Pathology.First series, Fascicle 1. Washington DC: AFIP; 2001: 149.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}