System: Skin: Adnexal: Neoplastic: Desmoplastic Trichoepithelioma

System: Skin: Adnexal: Neoplastic: Desmoplastic Trichoepithelioma

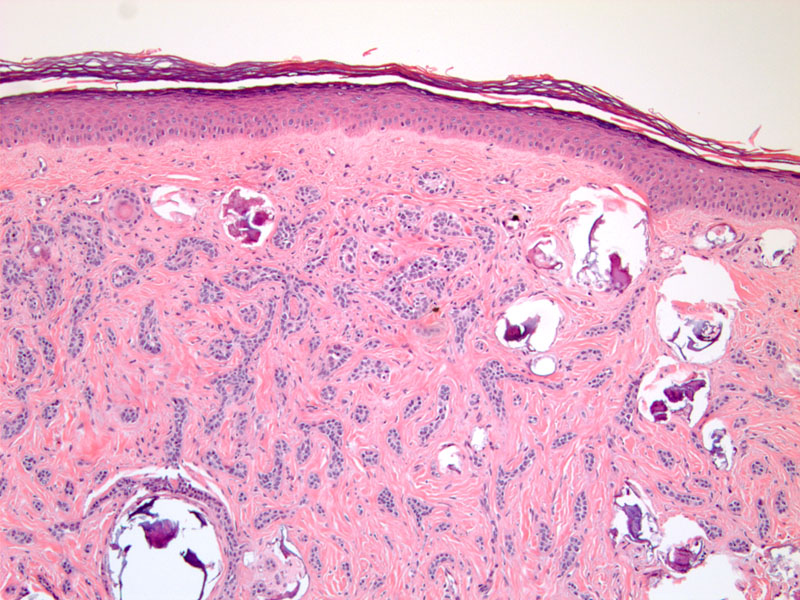
Case 1: Thin cords of bland basaloid cells interspersed throughout the dermis with scattered calcifications.
High power view shows the bland cytologic features of the basaloid cells surrounded by a dense fibrous stroma.
Desmoplastic trichoepithelioma is a distinct variant of trichoepithelioma (TE) that, like TE, is considered a benign neoplasm of follicular origin. Similarly, it is biphasic having both an epithelial and stromal component (fibroepithelial). What distinguished desmoplastic TE from conventional TE are thin strands of basaloid epithelial cells infiltrating the stroma. Similar to TE, desmoplastic TE has a dense fibrous stroma and may contain papillary mesenchymal bodies (clusters of fibroblasts adjacent to epithelial clusters), keratin horn cysts, and calcifications.
Differential diagnoses that should be considered include syringoma, basal cell carcinoma (especially the sclerosing and keratotic variants), and microcystic adnexal carcinoma. The latter two should be excluded given their malignant nature. Papillary mesenchymal bodies are a feature, that if present, are highly suggestive of trichoepithelioma (rarely present in keratotic BCC)(Brooke). Syringomas typically do not have horned cysts or calcifications, and clinically they are usually numerous rather than solitary. Features that are more suggestive of BCC include greater asymmetry in growth, deeper infiltration, nuclear atypia, solar elastosis, and stromal retraction artifact around basaloid cells. Differentiating microcystic adnexal carcinoma can be difficult, especially in superficial biopsies. If clear ductal differentiation is present, then microcystic adnexal carcinoma is likely.
Immunohistochemistry may have some use in delineating these lesions. CK20 or chromogranin can be useful to help distinguish TE from syringomas and microcystic adnexal carcinoma as it will highlight the follicular associated Merkel cells present in TE. Using IHC to differentiate TE from BCC may be of less clinical utility. CD10, CD34, bcl-2, Ber-Ep4, and stromelysin-3 have been cited in the literature as potentially markers, although the sensitivity and specificity is variable between studies and overall not that great (Swanson, Thewes, Weedon).
They usually present as a small (less than 1 cm), solitary lesions on the face that are hard and often have a depressed center. Women are more common affected than men.
If a definitive diagnosis of desmoplastic trichoepithelioma can be made in the initial biopsy specimen, no further treatment is needed as these are benign lesions. However, given that these lesions can be difficult to differentiate from basal cell carcinoma or microcystic carcinoma, resampling of scant shave biopsies may be necessary for a definitive diagnosis. As such, these lesions are often clinically treated like basal cell carcinoma with the goal of obtaining a negative margin.
These lesions are benign with no risk of progressing to carcinoma.
• Epidermis : Basal Cell Carcinoma, Infiltrating Type
• Lung : Lymphangioleiomyomatosis
• Adnexal : Microcystic Adnexal Carcinoma
Brooke JD, Fitzpatrick JE, Golitz LE. Papillary mesenchymal bodies: a histologic finding useful in differentiating trichoepitheliomas from basal cell carcinomas. J Am Acad Dermatol. 1989 Sep;21:523-8.
Swanson PE, Fitzpatrick MM, Ritter JH, et al. Immunohistologic differential diagnosis of basal cell carcinoma, squamous cell carcinoma, and trichoepithelioma in small cutaneous biopsy specimens. J Cutan Pathol. 1998 Mar;25(3):153-9.
Thewes M, Worret WI, Engst R, et al. Stromelysin-3: a potent marker for histopathologic differentiation between desmoplastic trichoepithelioma and morphealike basal cell carcinoma. Am J Dermatopathol. 1998 Apr;20(2):140-2.
Weedon D. Skin Pathology, 3rd ed. Philadelphia, PA: Elvsevier; 2010.
){kind=link}
){kind=link}