
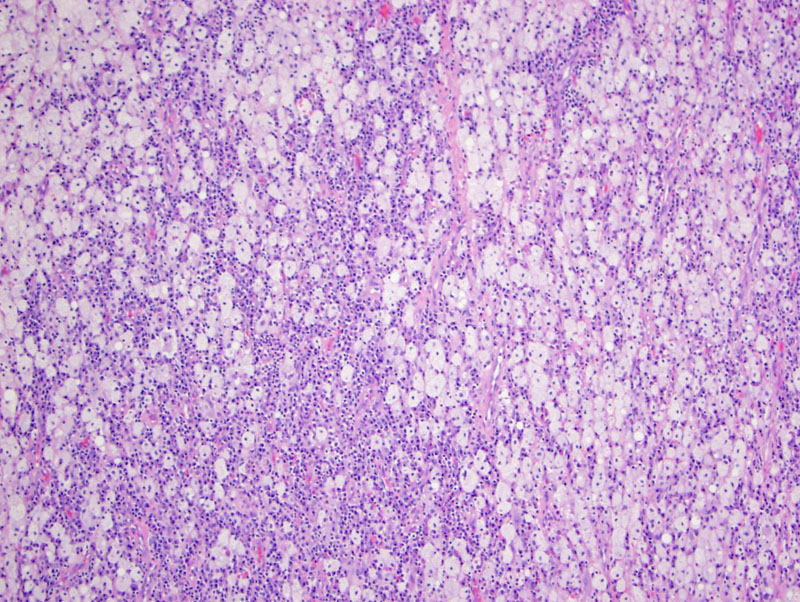
Sheets of histiocytes with lymphocytes and plasma cells were seen in this nasal specimen.
){kind=link}
A closer look at foamy cells (SHML cells) with interspersed inflammatory cells. In contrast to Langerhans cell histiocytes, the nuclei of SHML histiocytes do not have grooves or indentations.
){kind=link}
The histiocytes demonstrate emperipoiesis (phagocytosis of lymphocytes, plasma cells, RZBZCZs and neutrophils). The engulfed cells can be seen in the cytoplasm of the histiocytes.
){kind=link}
The histiocytes are strongly S100 positive. The cells are also positive for the histiocytic markers such as CD68, lyzozyme, CD163, HAM385 and MACH385; they are negative for CD1a and Langerin (Fletcher).
){kind=link}
Rosai–Dorfman disease, a.k.a. sinus histiocytosis with massive lymphadenopathy (SHML), is a rare, idiopathic and non-neoplastic disorder comprised of overproduction of histiocytes. SHML may present as a generalized process involving the lymph nodes or may present as extranodal disease. Cervical lymphadenopathy is most the commonly seen nodal site while the skin, upper respiratory tract, and the sinuses are the most common extranodal sites.
Within the head and neck, the nasal and paranasal sinuses are the most common location and the clinical presentation is that of a polypoid or nodular mass concerning for a neoplasm.
Rosai–Dorfman disease runs a benign course and the literature reports that treatment can vary from observation, corticosteroids, cytotoxic chemotherapy or radiotherapy. Surgical intervention may be considered for easily accessible masses or those impinging upon vital structures such as the airway.
In a review of 126 cases of (extranodal) sinonasal RDD (Chen et al, 2011), 32 (25.4%) had no recurrence or were alive with no evidence of disease; 69 patients (54.8%) had a recurrent, persistent, or progressive course; remission occurred in 1 patient (0.7%); and 6 patients (4.8%) died from the disease. There was no significant tendency for involvement of lymph nodes in patients with recurrent, persistent, and progressive disease.
→The head and neck is one of the most common extranodal sites affected by SHML.
→The SHML histiocytes are positive for S100 and histiocytic markers (e.g. CD68, lyzozyme), but negative for Langerhan cell markers (CD1a, Langerin).
• Lymph Nodes : Rosai-Dorfman Disease
• Dermis : Cutaneous Rosai-Dorfman Disease
Chen HH, et al. Factors associated with recurrence and therapeutic strategies for sinonasal rosai-dorfman disease. Head Neck. 2011 Aug 4. doi: 10.1002/hed.21832. [Epub ahead of print]
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 139.