System: Head and Neck: Sinonasal: Indeterminant: Schneiderian Papilloma, Fungiform (Exophytic) Type

System: Head and Neck: Sinonasal: Indeterminant: Schneiderian Papilloma, Fungiform (Exophytic) Type

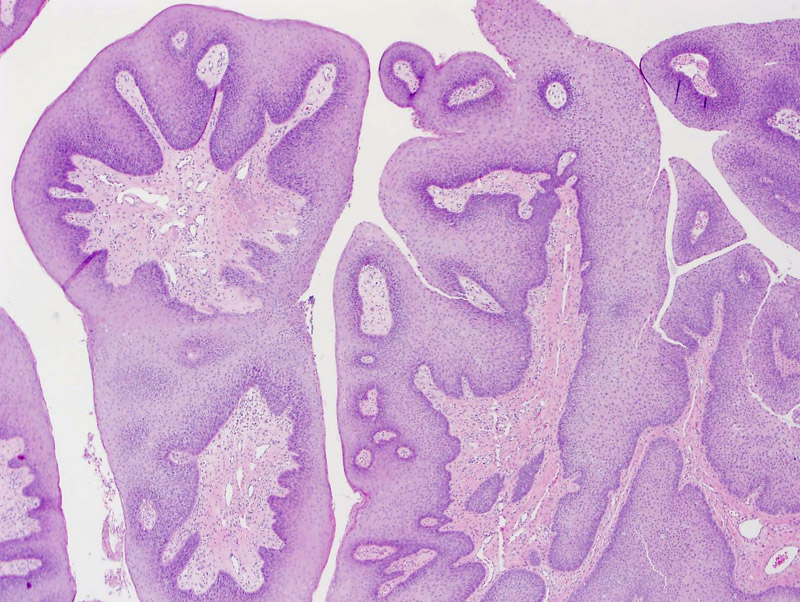
Case 1: Exophytic papillary growth typifies this the fungiform or exophytic type of Schneiderian papilloma.
Multilayered non-keratinizing squamous epithelium lines the undulations. There is minimal to absent atypia and the cells are well-polarized.
The sinonasal tract is composed of the nasal cavity and paranasal sinuses (maxillary, ethmoid, sphenoid, frontal) and nasopharynx is posterior and continuous with the sinonasal tract. Both cavities are lined by similar appearing respiratory epithelia containing minor salivary glands, however, it is important to note that there are major differences between to the two cavities that lead to distinct neoplasms native to that region.
For example, the sinonasal tract contains epithelia that is ectodermally derived, and the epithelia of the nasopharynx is endodermally derived. Thus, schneiderian papillomas arise almost exclusively in the sinonasal tract, and those rare cases that arise in the nasopharynx may be due to ectopic ectodermal rests from the sinonasal tract. Nasopharyngeal carcinomas arise in the nasopharynx and endodermally-dervied squamous papillomas are most commonly seen in the oral cavity and larynx (Fletcher).
There are three distinct subtypes of schneiderian papillomas: fungiform (a.k.a. septal, exophytic), inverted, and oncocytic. The inverted type is the most common subtype (62%), followed by the fungiform (32%) and oncocytic (6%)(Barnes). These all tend to be unilateral.
The fungiform type tend to occur in a younger age group (20-50 years), whereas the inverted and oncocytic types affect an older population (40-70 years). There in a male predominance in the fungiform and inverted types, whereas the gender distribution is equal in the oncocytic type. The fungiform type arises predominantly in the nasal septum whereas the inverted and oncocytic types arise in the lateral nasal walls and sinuses.
HPV subtypes 6 and 11 are found in approximately half the cases in the fungiform and inverted types, whereas this association is absent in the oncocytic type. An association with EBV has not been established. Malignant transformation is largely absent in the fungiform types, and occurs in 2-27% of the inverted types and 4-17% of the oncocytic types.
Histologically, the fungiform type shows a papillary exophytic growth, and is composed with non-keratinzed bland polarized epithelium. Scattered mucocytes and microcysts may be present. This is in contrast with a endodermally-derived squamous papilloma, which would not contain intraepithelial mucocytes (Fletcher).
The fungiform type is 2-10 times more common in men. They arise in the nasal septal with only a minority of cases being described in the lateral nasal wall. Symptoms include airway obstruction, epistaxis, or pain (Barnes).
→Male predominance, 50% are HPV 6 or 11 positive, arises in the nasal septum and rarely transforms into a malignant tumor.
Barnes L. Schneiderian Papillomas and Nonsalivary Glandular Neoplasms of the Head and Neck. Mod Pathol 2002;15(3):279-297.
Fletcher CDM, ed. Diagnostic Histopathology of Tumors. 3rd Ed. Philadelphia, PA: Elsevier; 2007: 83-7.
){kind=link}
){kind=link}