System: Skin: Adnexal: Neoplastic: Reticulohistiocytoma

System: Skin: Adnexal: Neoplastic: Reticulohistiocytoma

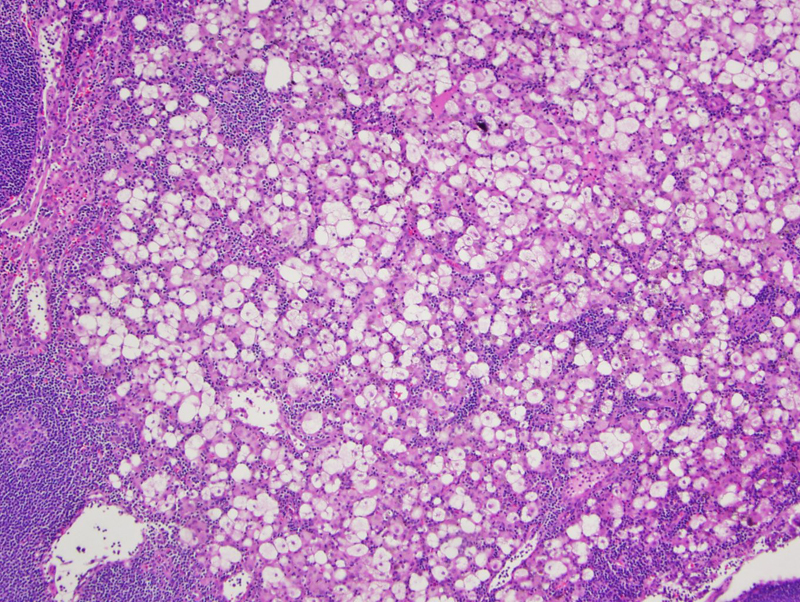
Case 1: Low power view showing large epithelioid cells wtih some adjacent lymphocytes in the upper/mid dermis.
Medium power showing abundant pale cytoplasm of histiocytes. While this case shows the histiocytes to have pale cytoplasm, it is more characteristic for the histiocytes to have a 'ground glass' effect with a finly granular, eosinophilc cytoplasm.
High power view of a mix of histiocytes demonstrating both vacuolated and xanthomatized features.
Reticulohistiocytoma was first reported by Zac in 1950. It is now suggested that these lesions be classified as Solitary Epithelioid Histocytoma (SEH) as this term more accurately reflects their cytomorphology and immunophenotype (Miettinen). While the exact etiology of these lesions remains unclear, Miettinem suggest that these lesions represent a localized, cytokine-induced collection of histiocytes secondary to an unknown inflammatory stimulus.
Histologically, reticulohistiocytomas demonstrate a dermal inflammatory infiltrate composed primarily of histiocytes and lymphocytes, and to a lesser extent plasma cells and eosinophils. The histiocytes are both mono- and multinucleated and have a characteristic abundant eosinophilic, finely granular cytoplasm crating a ‘ground glass’ effect. The histiocytic immunophenotype is positive for lysozyme, CD68, and CD 163. S100 is usually negative.
Individuals typically present with a single, skin colored to yellow, superficial papule or nodule that is usually less than 1 cm. Lesions have a predilection to occur on the head, but may occur on any cutaneous site. Young adults are more commonly affected and there is a slight male predominance.
The clinical spectrum ranges from a single lesion to multicentric reticulohistiocytosis with systemic involvement. Individuals with multicentric reticulohistiocytosis often have associate arthropathy, with the interphalangeal joints of the hands most commonly affected. Hyperlipidemia, positive PPD, systemic vasculitis, and autoimmune disease are all associated with the systemic reticulohistiocytosis. Interestingly, approximately 1/3 of patients have an underlying malignancy (Bolognia).
Surgical excision is curative for single nodules, although many individual nodules resolve on their own. Treatment of systemic reticulohistiocytosis is more complicated with little proven to be effective.
Individuals with a solitary lesion are typically healthy and the lesion usually resolves on its own.
Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. St. Louis, MO: Mosby; 2008.
Miettinen M, Fetsch JF. Reticulohistiocytoma (solitary epithelioid histiocytoma): a clinicopathologic and immunohistochemical study of 44 cases. Am J Surg Pathol. 2006;30:521-8.
Zak FG. Reticulohistiocytoma (‘ganglioneuroma’) of the skin. Br J Dermatol. 1950;62:351–35.
){kind=link}
){kind=link}
){kind=link}