System: Hematopathology: Lymph Nodes: Neoplastic: Angioimmunoblastic T Cell Lymphoma

System: Hematopathology: Lymph Nodes: Neoplastic: Angioimmunoblastic T Cell Lymphoma

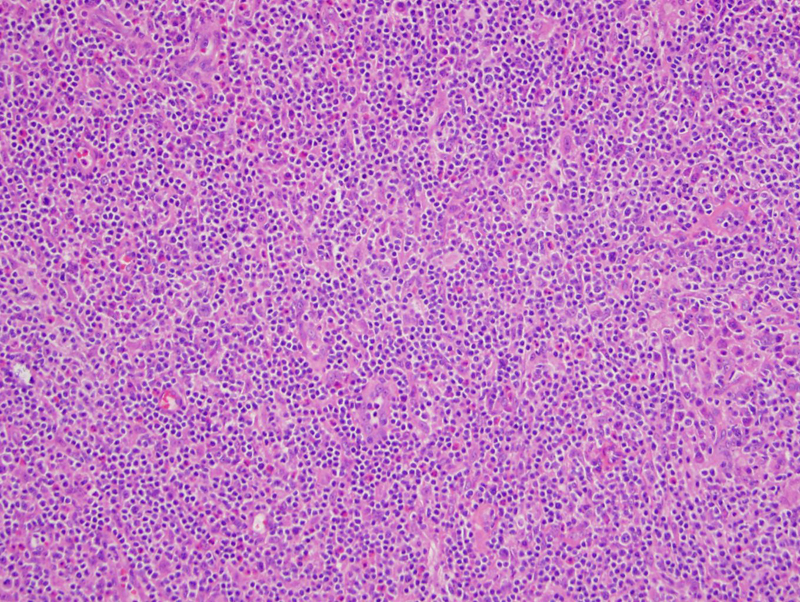
The nodal architecture is effaced by a diffuse lymphoproliferative process.
Proliferative high endothelial vessels are prominent. Though difficult to detect at this magnification, the neoplastic T-cells have clear to pale cytoplasm and generally cluster around the vessels.
Angioimmunoblastic T-cell lymphoma occurs primary in the lymph nodes. AITL is characterized by neoplastic T-cells, proliferation of high endothelial venules, disrupted and proliferated follicular dendritc cell networks and EBV positive B-cell immunoblasts.
The neoplastic T-cells tend to have clear or pale cytoplasm and show the usual T-cell markers (CD2, CD3, CD5, CD7), however, loss of one of these markers is not unusual. Furthermore, the T-cells also aberrantly express CD10 (usually a germinal center marker) and chemokin CXCL13. The proliferated and disrupted follicular dendritic cell networks can be highlighted by CD21 or CD35.
Although the majority of AITL demonstrate EBER positivity in B-cell immunoblasts, the role of EBV in pathogenesis has not been clearly delineated yet. 75% of AITL cases will demonstrate clonal rearrangement of TCR genes.
Patients are middle-aged or older. Common clinical presentation includes generalized lymphadenopathy, fever, weight loss, hypergammaglobulinemia and a skin rash.
→A nodal T-cell lymphoma that exhibits T-cell markers as well as CD10 and CXCL13.
→Histologically, clusters of "clear" T-cell immunoblasts cluster around proliferated high endothelial venules.
→A disrupted and expanded dendritic cell network can be highlighted by dendritic cell markers.
→The background B-cell immunoblasts are EBER positive.
){kind=link}
){kind=link}