System: Skin: Adnexal: Neoplastic: Poroma

System: Skin: Adnexal: Neoplastic: Poroma

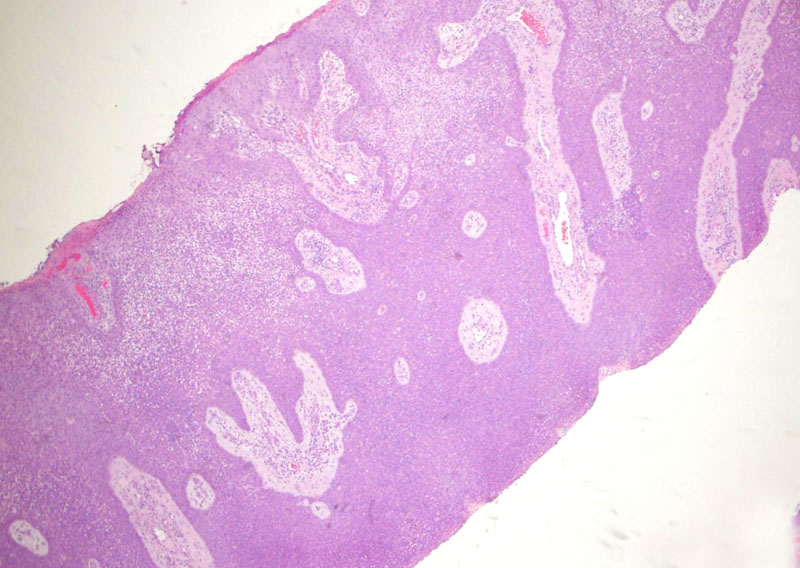
Case 1: A proliferation of so-called poroid cells is seen extending from the epidermis to the superficial dermis, with broad-based connections to the epidermis. At low power, one might be reminded of a seborrheic keratosis.
The neoplastic poroid cells are basaloid and cuboidal. Although not obvious in this case, usually there are scattered sweat glands lined by cuboidal cells within the tumor.
Another look at the poroid cells with small bland nuclei and cytoplasm that can range from eosinphilic to clear and glycogenated.
A poroma is an adnexal neoplasm composed of basaloid and cuboidal "poroid" cells, that is cells with glandular/ductal differentiation. Poromas have been considered to be of eccrine origin, however, current investigation reveals that sweat gland neoplasms can be of either eccrine or apocrine origin (Obaidat, McCalmont). Either way, this is not clinically significant.
There are several variants of poromas which depend on the the location of the tumor. For example, a poroma involves both the epidermis and dermis, whereas a hidroacanthoma simplex (a.k.a intraepidermal poroma) is confined to the epidermis and a dermal duct tumor is confined to the dermis with no epidermal attachments (Obaidat).
Histologically, there is fairly solid proliferation of "poroid" cells, which are cuboidal and basaloid. The neoplastic cells are often sharply demarcated from adjacent normal epithelium, and form "broad-based" connections to the epidermis. The tumor will extend into the superficial dermis. Scattered smalls sweat ducts lined by cuboidal epithelium are usually seen within the tumor. Occasionally, the poroid cells may contain plentiful melanin, so-called pigmented poroma.
Differential Diagnosis:
In a porocarcinoma (a.k.a. malignant eccrine poroma), the neoplastic poroid cells have increased nuclear atypia, hyperchromasia and prominent nucleoli.
In a hidradenoma, the neoplastic cells can be similar and this tumor also has scattered sweat glands, however, hidradenomas usually are confined in the upper dermis and only a minority of cases have epidermal connections (Obaidat). Furthermore, it seems to me that hydradenomas exhibit more clear cell change with clear cells having a prominent cell membranes (a "vegetable" or plant-like look) whereas the neoplastic cells in poromas are more uniformaly basaloid. If you don't agree, please send us an email. Otherwise, a dermal based poroma (dermal duct tumor) and hidradenoma (based in the dermis) seem pretty synonymous.
Usually occurs in adults with a predilection for the soles, palms and less commonly, head, neck and trunk. Clinically, they present as friable papules or plaques, resembling a pygenic granuloma (Obaidat, Rapini). Multiple poromas can be disabling, especially if they occur on the soles (McCalmont).
• Epidermis : Seborrheic Keratosis
McCalmont T. Poroma: eMedicine. Last updated Jan 12 2012: Available at: emedicine.medscape.com/article/1057014
Obaidat NA, et al. Skin adnexal neoplasms - part 2: An approach to tumors of cutaneous sweat glands. J Clin Pathol 2007;60:145-9.
Rapini RP. Practical Dermatopathology. Philadelphia, PA: Elsevier; 2005: 300.
){kind=link}
){kind=link}
){kind=link}