
Melanocytic nests can be junctional, dermal or compound (as seen here). Clefts are common around the nests. There can be pagetoid spread of melanocytes.
){kind=link}
The morphology of the melanocytes are epithelioid and/or spindled (thus, the antiquated term spindle and epithelioid cell nevus). A Kamino body can be seen at about 9 o'clock.
){kind=link}
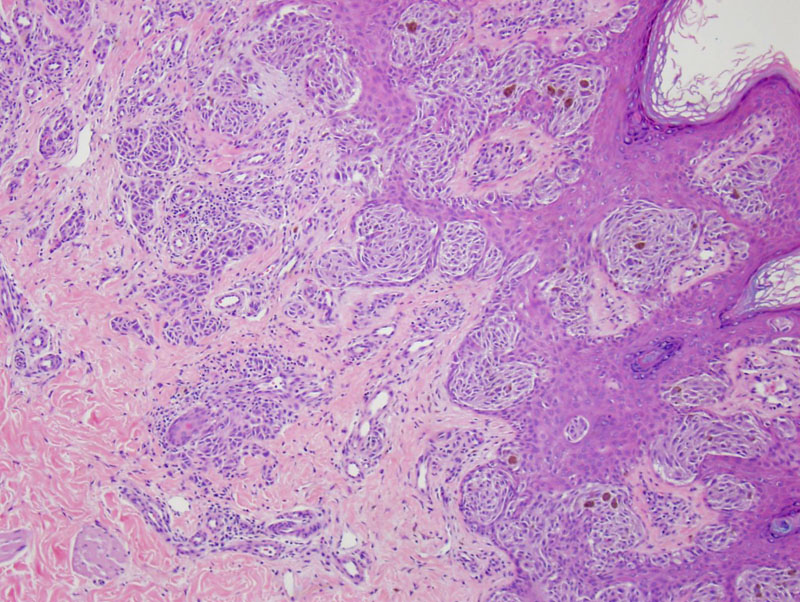
A higher power demonstrates epithelioid nests; there is a hint of maturation of melanocytes in the deeper portions of the lesion. In these cases, HMB-45 (present only in immature melanocytes) would demonstrate zonal reactivity.
){kind=link}
The Spitz nevus has also been referred to as a spindle or epithelioid cell nevus and a benign juvenile melanoma. Generally, this diagnosis can be made fairly easily on nevi removed from children, especially those located on the face.
However, one of the biggest concerns and most challenging tasks when making the diagnosis of Spitz nevi is to distinguish it from melanoma, which can have a similar histologic appearance. Unfortunately, this is not always the easiest task for a general surgical pathologist. Therefore, caution should be used when making this diagnosis, especially in adults, as the incidence of Spitz nevi decreases after the age of 25 (Silverberg).
Spitz nevi are most commonly compound, but they can be junctional or intradermal as well. The cells can be either spindle-shaped or epithelioid with abundant eosinophilic cytoplasm. Characteristics that favor a Spitz nevus over a Spitzoid melanoma are: small size, well circumscribed, maturation of melanocytes, Kamino bodies (eosinophilic globules near the border of the dermis and epidermis), absence of deep dermal mitotic figures (occasional superficial dermal mitoses are okay), clefting around nests and at the dermal epidermal junction, and epidermal hyperplasia.
Ancillary tests that can be used to help distinguish Spitz nevi from melanoma include CGH and FISH. Bastani showed that up to 25% of Spitz nevi have an increase number of chromosome 11p that has not been shown to occur in melanoma. On the other hand, melanoma has been shown to have numerous chromosomal alterations including deletions of 9p, 10q, 6q and additions of 7, 8, and 6p (Bastani, Busman).
Most commonly present rapidly as a tan, skin colored, or red well circumscribed papule on the face of a child or teenager. Spitz nevi can be pigmented and have been reported to occur on the extremities and trunk. One clinical feature that can be used to help distinguish Spitz nevi from melanoma is the age at presentation as Herreid et al. showed the average age for Spitz nevi is 21 years (range 6 months to 72 years) and 56 years for melanoma (range 18 to 94 years).
Complete surgical resection with negative margin is important because of the difficulty of classifying these lesions. Patients that have nevi with atypical features are advised to have a 1cm negative margin and should be closely monitored for signs of recurrence.
Spitz nevi are benign melanocytic lesions that generally do not recur once excised. Data regarding the outcomes of patients with atypical Spitz nevi are more limited as there is no precise diagnostic criteria and debate among a lot of dermatopathologist as how to classify these lesions.
Bastian B, Wesselmann U, Pinkel D, et al. Molecular cytogenetic analysis of Spitz nevi shows clear differentiation to melanoma. J Invest Dermatol. 1999;113:1065–9.
Busam KJ. Dermatopathology: Foundations in Diagnostic Pathology 1st Ed. Philadelphia, PA: Elsevier; 2010.
Herreid PA, Shapiro PE. Age distribution of Spitz nevus vs malignant melanoma. Arch Dermatol. 1996;132:352-3.
Silverberg SG. Silverberg's Principles and Practice of Surgical Pathology and Cytopathology. Philadelphia, PA: Elsevier; 2006:278-9.