System: Gastrointestinal: Liver: Developmental: Extrahepatic Biliary Atresia

System: Gastrointestinal: Liver: Developmental: Extrahepatic Biliary Atresia

Proliferation of ductules is seen at the port of the parenchyma and portal tracts; portal edema is not prominent because this patient has been affected for 2 months. Image
ductular cholestasis is seen with ductal structures plugged with insippated bile Image
lobular cholestatis Image
An expanded portal tract shows ductual reaction occurs within portal tracts and along the outside of the lobules Image
portal fibrosis is seen expanding the triads; a minimal degree of periportal fibrosis is present. this infant had choledochocal cyst obstruction for 2 months; it takes months for true septal fibrosis to develop, and years for secondary biliary cirrhosis to form. Image
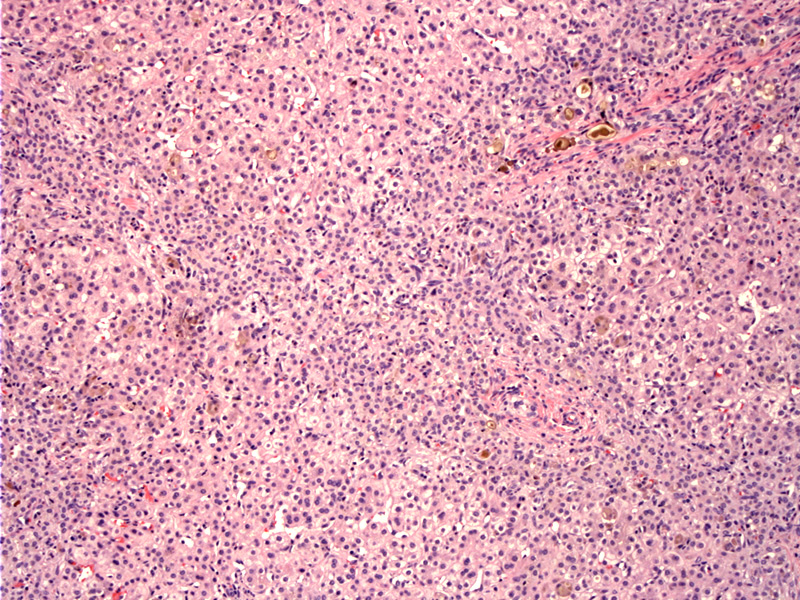
Case 2 - newborn with markedly elevated bilirubin and absense of bile ducts and giant cell transformation with gigantic hepatocytes Image
no ducts but lots of ductular proliferation at the edge of the lobule Image
fiborosis too Image
another case Image
21 Image
again Image
corresponding trichrome Image
Infants develop jaundice by the second or third week of life. The infant may gain weight for the first month, but then lose weight and become irritable with worsening jaundice.
Treatment involves the Kasai procedure, which connects the liver to the small intestine, circumventing the abnormal ducts.
60% of children achieve biliary drainage after Kasai portoenterostomy and have serum bilirubin within the normal range within 6 months. 80% of children who attain satisfactory biliary drainage reach adolescence with a good quality of life without undergoing liver transplantation.
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}