
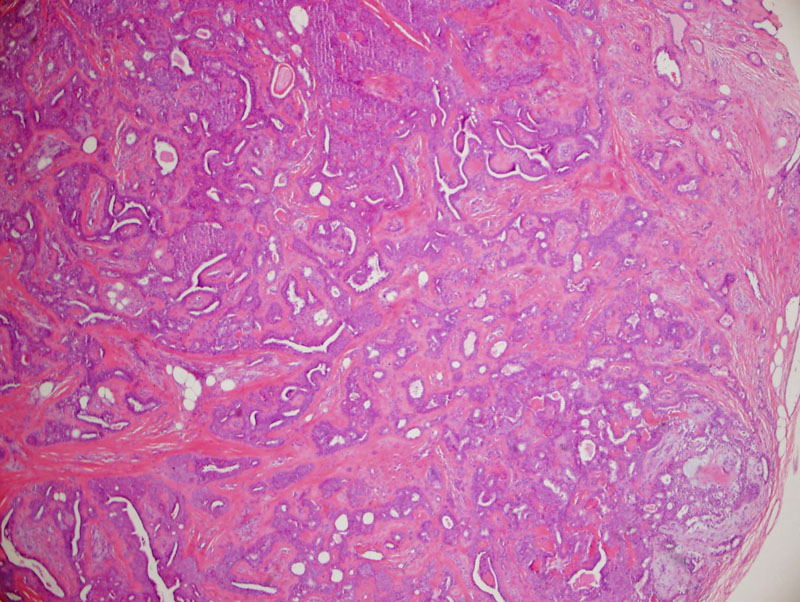
A fairly well demarcated nodule situated in the dermis composed primarily of epithelial and mesenchymal (myxoid, chondroid, fibrous stroma) components.
){kind=link}
The epithelial component forms nests and tubules. Some experts believe that chondroid syringomas arise from apocrine structures, and thus, one may see the sweat ducts lined by two epithelial cells (recapitulating apocrine sweat glands)(Paik).
){kind=link}
Approximately half of these tumors have mature hyaline cartilage present in the stroma (Bolognia).
){kind=link}
Higher power view showing myoepithelial cells swirling in the mxyochondroid stroma.
){kind=link}
Benign mixed tumor (a.k.a. chondroid syringoma) is a tumor so-named because of the presence of both epithelial and mesenchymal components. Dr. Rapini thinks this appellation is "ludicrous" because most epithelial neoplasms have a stromal component, however, he points out that the stroma in chondroid syringoma/benign mixed tumor is strikingly cartilaginous (Rapini).
Histologically, the epithelial cells form nests, cords or ductal structures and are eosinophilic. The stromal cells demonstrate myoepithelial differentiation. The stroma is bluish, mucinous and chondroid. Scattered horn cysts may also be seen. Chondroid syringoma is classified as eccrine or apocrine type, depending on the appearance of the sweat gland lumina (Obaidat).
Mixed tumors of the skin and mixed tumors of salivary gland origin (pleomorphic adenoma) share a similar appearance under the microscope, but it is important to note that they have different clinical courses. Mixed tumors of the skin are indolent and rarely recur after excision. On the other hand, pleomorphic adenomas of the salivary gland have a tendency to recur and may progress to malignancy (carcinoma ex pleomorphic adenoma).
Clinically, these lesions present as shiny or waxy, firm, solitary, nodules most often located on the head and neck of the middle-aged and elderly.
Most lesions are treated by enucleation or surgical resection.
Cutaneous mixed tumors are benign and have little capability of proliferating. Once treated, it is unlikely for the lesion to recur. Malignant chondroid syringoma has been described but it is extremely rare, and may arise de novo or from a pre-existing chondroid syringoma. This malignant form is characterized by cellular atypia, increased mitotic activity and infiltrative margins (Obaidat).
Bolognia JL, Jorizzo JL, Rapini RP, eds. Dermatology. St. Louis, MO: Mosby; 2008: 1696.
Hirsch P, Helwig EB. Chondroid syringoma. Mixed tumor of skin, salivary gland type. Arch Dermatol 1961 Nov;84:835-47.
Obaidat NA. Skin adnexal neoplasms - part 2: An approach to tumors of cutaneous sweat glands. J Clin Pathol 2007;60:145-159.
Paik YS, Liess BD. Chondroid syringoma of the scalp: case report and discussion of clinical features, histopathology, and treatment. Ear Nose Throat J. 2011 Apr;90(4):190-1.
Rapini RP. Practical Dermatopathology. Philadelphia, PA: Elsevier; 2005: 302.
Rosai, J. Rosai and Ackerman’s Surgical Pathology, 10th Ed. Philadelphia, PA: Elsevier; 2011:139.