
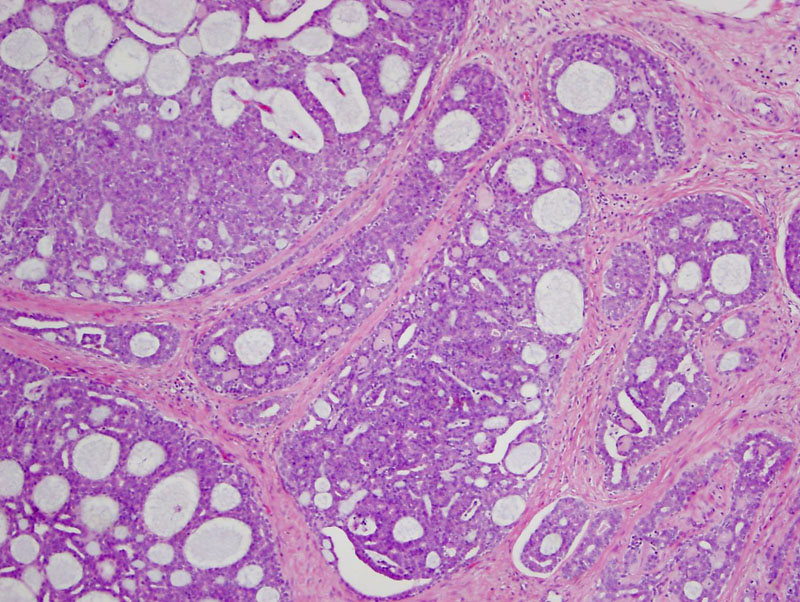
The tumor shows the classic appearance of adenoid cystic carcinoma, characterized by lobular collections of deeply basophilc cells with a cribriform pattern; however, the site of this excision was the scalp.
){kind=link}
At higher power, one can appreciate the nice cribriform spaces and some extra basement membrane deposition. The cystic spaces are often occupied by mucin that is either eosinophilic PAS-positive or basophilic with a granular appearance. Perineural invasion is a common feature of this tumor, occurring in up to 76% of cases (Naylor).
){kind=link}
Adenoid cystic carcinoma most commonly occurs in the salivary gland, but have been reported in the breast, trachea, bronchi, uterus, prostate, lacrimal gland, external ear canal, and skin (Naylor, Rosai). Primary cutaneous adenoid cystic carcinoma is very rare and according to a 2008 literature review conducted by Barnes, only 61 have been reported in the literature.
The diagnosis of primary cutaneous adenoid cystic carcinoma can be made after metastatic disease from the salivary gland has been excluded.
Primary cutaneous adenoid cystic carcinomas (PCACC) usually occur as firm, poorly circumscribed, slow growing, skin-colored nodules. Men and women are equally affected with a mean age at presentation of 59 years (Naylor). The most common location of PCACC is the scalp (41% of PCACC cases), but other sites include the chest, abdomen, back, eyelid, and perineum.
Wide surgical resection of the tumor with negative margins is the standard of care. Some patients receive adjuvant radiation and/or chemotherapy.
In the salivary gland, prognostic factors for adenoid cystic cardinoma include stage, location of the tumor and histologic subtype (cribriform, tubular, solid). The solid pattern has the worst prognosis, a fact corroborated by a high incidence of aneuploidy and overexpression of p53 seen in this particular subtype. Adenoid cystic carcinoma of the salivary gland generally has a poor prognosis with frequent pulmonary metastases (Naylor).
On the other hand, adenoid cystic carcinoma of the breast and lung usually has a more favorable prognosis. Adenoid cystic carcinomas in these locations are quite indolent, with rare metastases and but common local recurrences. Primary cutaneous adenoid cystic carcinoma appears to belong to this more indolent group, however local recurrence is common (Naylor).
• Invasive Carcinoma - Special Types : Adenoid cystic carcinoma
• Sinonasal : Adenoid Cystic Carcinoma (Case 2)
• Lung : Adenoid Cystic Carcinoma
• Salivary Gland : Adenoid Cystic Carcinoma
Barnes J, Garcia C. Primary cutaneous adenoid cystic carcinoma: a case report and review of the literature. Cutis. 2008 Mar;81(3):243-6.
Boggio R. Adenoid cystic carcinoma of scalp [letter]. Arch Dermatol. 1975;111:793-4.
Naylor E, Sarkar P, Perlis CS, Giri D, Gnepp DR, Robinson-Bostom L. Primary cutaneous adenoid cystic carcinoma. J Am Acad Dermatol. 2008;58:636-41.
Dores GM, Huycke MM< Devesa SS, Garcia CA. Primary cutaneous adenoid cystic carcinoma in the United States: incidence, survival, and associated cancers, 1976 to 2005. J Am Acad Dermatol. 2010;63:71-8.
Rosai, J. Rosai and Ackerman’s Surgical Pathology, 10th Ed. Philadelphia, PA: Elsevier; 2011: 142, 833-5.