
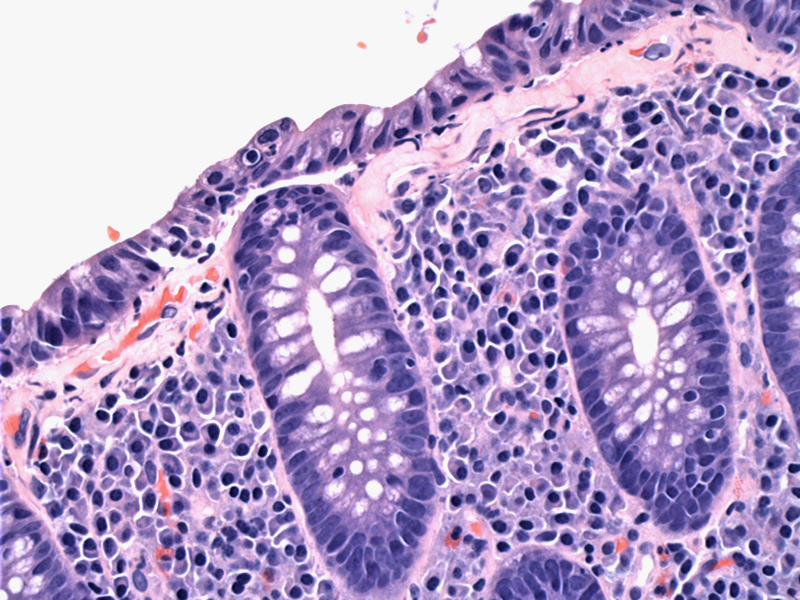
Diagnosis of collagenous colitis also requires the findings of mucosal injury. Higher power reveals increased superficial plasma cells underlying a damaged surface epithelium. The surface epithelium often lifts off the basement membrane. Note the intraepithelial lymphocytes.
){kind=link}
Trichrome staining highlights the thickened subepithelial basement membrane. This is due to collagen deposition, which tends to encircle and entrap the subepithelial capillaries, thus creating a ragged and irregular lower border to this collagen stripe. Normally, the basement membrane is 2-5 microns thick, while in collagenous colitis, the thickness increases to 10-70 microns, with 30 microns being the most reliable thickness in establishing the diagnosis.1,2
){kind=link}
This example is more challenging. While there is an intraepithelial lymphocytosis, there are also scattered eosinophils, which is more likely in collagenous colitis over lymphocytic colitis.
){kind=link}
The corresponding Trichrome shows some entrapped capillaries within the basement membrane. Collagen strands percolate down from the basement membrane.
){kind=link}
The broader category of microscopic colitis includes lymphocytic colitis and collagenous colitis, in which patients suffer from chronic nonbloody diarrhea, but colonoscopy findings are normal. However, under the microscope, one finds evidence of increased intraepithelial inflammation and surface damage, hence the term microscopic colitis.
There have been cases that demonstrate lymphocytic colitis evolving into collagenous colitis, with the subepithelial deposition as a late presentation of the disease as a response to continued inflammation and fibrosis.2 Thus, it is theorized that an underlying immune dysfunction leads to microscopic colitis, and lymphocytic and collagenous colitis are variations in presentation of the same disease process. Both conditions are associated with other autoimmune disorders, with degenerative osteoarticular disease and celiac disease being the most common.1,2 There may also be an association with smoking and use of NSAIDs.1,2
Age range of 23-86 (mean age of 54-66 years); strong female predilection (M:F=1:10). Presents with chronic watery diarrhea, colicky abdominal pain and normal endoscopy. Remissions and relapses are common. Preferentially affects the proximal bowel, while the distal bowel (left colon and rectum) may be spared.
Anti-inflammatory medications
Benign; may spontaneously resolve. Diverting the fecal stream causes resolution of disease in some cases.
1 Iacobuzio-Donahue CA, Montgomery EA. Gastrointestinal and Liver Pathology: Foundations in Diagnostic Pathology. Philadelphia, PA: Elsevier; 2005: 327-9.
2 Fenoglio-Preiser CM, et al. Gastrointestinal Pathology: An Atlas and Text. 3rd Ed. Philadelphia, PA: Lippincoott Williams & Wilkins; 2008: 843-5.